Abstract
This colorectal case study was part of a joint study conducted by Wisconsin Diagnostic Laboratories, Rosalind Franklin University, and Cision Vision Inc. InVision is an optical device that provides enhanced contrast between lymph nodes and surrounding adipose tissue based upon differing chemical compositions in real-time without the use of radiation or contrast media.1
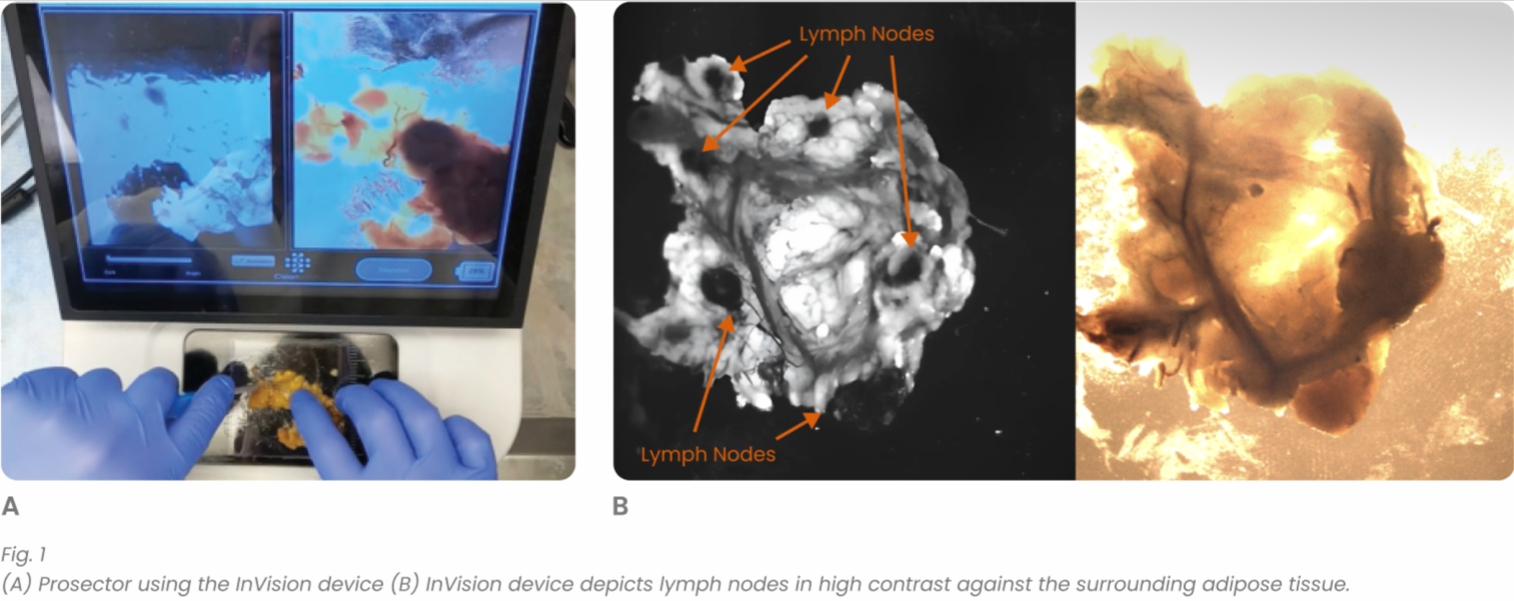
Through use of Cision Vision’s innovative technology, InVision (Fig. 1), lymph node yield drastically improved. Consequently, with the increase in lymph node yield, the pN (N-regional lymph node) category of the American Joint Committee on Cancer (AJCC) Tumor, Node, Metastasis (TNM) staging system was impacted.
Introduction
Lymph node retrieval in surgically excised specimens is one of the most challenging tasks completed in anatomic pathology. It can take a prosector multiple hours to finish a single lymph node search. When such searches are inadequate and the established minimums for lymph node count are not met, re-grossing is required which prolongs turnaround time for a case. Lymph node yield is of significant clinical consequence for cancer patients. Decades of clinical evidence has shown a strong correlation between the number of lymph nodes examined and patient survival.2 Therefore, prosectors are encouraged to find all the lymph nodes in each relevant specimen regardless of the time it takes and challenges it creates. This problem has also been exacerbated by the recent advent of neoadjuvant chemotherapy which shrinks the size of lymph nodes making them more difficult to find, particularly for colorectal cancer cases.
Cision Vision’s InVision product is a novel imaging device that depicts lymph nodes in high contrast against the surrounding adipose tissue.1 This is done in real-time without the need for injections or radiation. The technology was developed at the Massachusetts Institute of Technology (MIT) by Drs. Angela Belcher and Jeremy Li. It utilizes shortwave infrared light that exploits the natural water content differences which exist between lymph nodes and fat.3 Lymph nodes are high in water content. Therefore, they absorb the shortwave infrared light and appear dark on imaging. This is in contrast to adipose tissue which has a low water content and reflects light, appearing bright on imaging. Aided by the real-time visualization of lymph nodes, a prosector can palpate and dissect the tissue directly on top of the InVision imaging platform. Therefore, the prosector’s tactile skills are reinforced by the real-time visual feedback provided by the InVision device.
In this case study, the effectiveness of the InVision device was evaluated by comparing it to the results of manual palpation from a Pathologists’ Assistant (PA) with 20 years of grossing experience. The PA manually palpated the specimen and searched for lymph nodes. The lymph nodes retrieved during this step were gathered and labeled as the first batch. The PA then went through the remaining adipose tissue scanning it with use of the InVision device to see if there were additional lymph nodes that were missed during the initial, manual palpation step. If lymph nodes were found by scanning with the InVision device, these lymph nodes were submitted as a second batch. The numbers of lymph nodes in both batches are confirmed through routine histologic examination. Comparison of the lymph node counts between the two batches provided insight into the effectiveness of the InVision device for lymph node retrieval.
Case History
A 46-year-old Caucasian male presented to his general practitioner (GP) with complaints of persistent, nonspecific pelvic pain. Family history was unremarkable for rectal cancer and no associated risk factors were reported. Subsequently, the patient was referred for MRI which revealed suspected adenocarcinoma of the rectum that was clinically staged as IVA (cT3, cN1b, cM1). The primary mass was circumferential, 2.1 cm on imaging, and located 6 cm from the anal verge with mesorectal fascia involvement (MRF+), and suspicious mesorectal and presacral lymph nodes. A solitary liver mass was also present, measuring 1.5 cm in greatest dimension. Biopsies were taken of the both the rectal and liver masses. The rectal mass biopsy revealed moderately differentiated adenocarcinoma and the liver mass biopsy revealed adenocarcinoma compatible with a rectal primary. After initial diagnosis, the patient received combination neoadjuvant therapy which consisted of FOLFIRINOX+Avastin and short course radiation over 4 consecutive days. Upon completion of the aforementioned therapy, the patient underwent a low anterior resection (Fig. 2) in conjunction with a hepatic wedge excision of segments 7 and 8.

Pathologic examination of the low anterior resection was completed via use of the Quirke method. This method of prosection allows for thorough visualization of the tumor in relation to the mesorectal/circumferential radial margin (CRM) by leaving the specimen intact within the area of the mass. This area is serially sectioned from proximal to distal at 3 to 5 mm intervals and the corresponding sections are subsequently referred to as levels. Sectioning of this case revealed a 2.5 x 1.3 x 0.3 cm centrally ulcerated, endophytic, tan mass within levels 2-5 (Fig. 3). The mass measured 0.6 cm from the distal margin, 18.5 cm from the proximal margin, 0.8 cm from the anterior mesorectal margin and extended below the peritoneal reflection with focal infiltration into the muscularis propria.

As for the lymph node search, 19 lymph nodes were identified in total, 8 via use of traditional manual palpation by the prosector and 11 via use of the InVision device. Two out of eight lymph nodes found were microscopically positive for metastatic adenocarcinoma from the manual palpation batch;
1 out of 11 nodes were microscopically positive from the batch retrieved with assistance from the InVision device.
As for the lymph node search, 19 lymph nodes were identified in total, 8 via use of traditional manual palpation by the prosector and 11 via use of the InVision device. Two out of eight lymph nodes found were microscopically positive for metastatic adenocarcinoma from the manual palpation batch;
1 out of 11 nodes were microscopically positive from the batch retrieved with assistance from the InVision device.
Due to the fact that only 8 lymph nodes were found through the traditional manual palpation method, which falls short of the established minimum of 12 stipulated by AJCC and the College of American Pathologists (CAP), this case would be subject to re-grossing.
With the assistance of InVision, the total number was increased to 19, a 137.5% increase in lymph node count, bringing it into compliance with lymph node yield requirements. More importantly, because one additional positive lymph node was found, the patient’s N category was upstaged from ypN1a to ypN1b (Fig. 4).2 The final diagnosis was residual invasive moderately differentiated adenocarcinoma of the rectum without involvement of the margins and metastatic adenocarcinoma with extensive liver necrosis, consistent with metastasis from a rectal primary. The pathologic stage was reported as ypT2 pN1b PM1a.
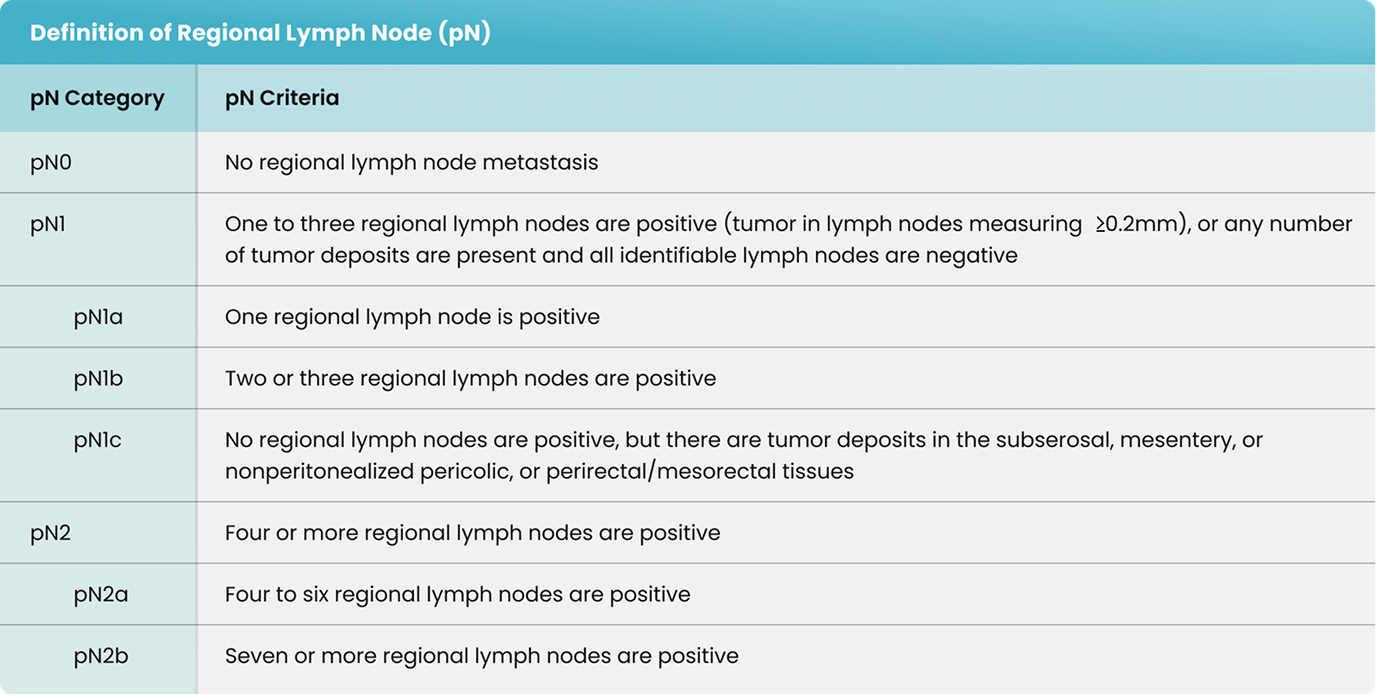
Fig. 4 AJCC TNM staging for colorectal carcinoma with specific information related to N categorization.
Discussion
Colorectal cancer staging utilizes the TNM system established by AJCC. Pre-fix “p” designates pathologic stage while “c” denotes clinical stage. Cases staged subsequent to use of neoadjuvant therapy utilize the pre-fix “yp”. These designations are important for QA/QC purposes across professions. As with any cancer, as the stage increases, patient prognosis inevitably decreases.
A minimum number of regional nodes is needed for accurate N category staging and is recommended by the National Comprehensive Cancer Network (NCCN) and accepted by the AJCC and CAP (Fig. 4).4 The minimum number of lymph nodes determined to be adequate for accurate colorectal cancer staging is 12. For reasons unknown, an association has been found between examination of 12 or more lymph nodes and improved patient survival.4
Additionally, as outlined in the Intergroup Trial INT – 0089, conducted by Le Voyer TE, Sigurdson ER, Hanlon AL, et al., an increase in the number of lymph nodes examined correlated with an increase in survival in patients with node negative and node positive disease.5 These findings highlight the importance of lymph node yield for accurate N category staging and predictions related to patient survival.
Use of the novel InVision device, in this instance, upstaged the patient from ypN1a to ypN1b and improved lymph node yield by 137.5%. By doing so, correlation within the N category between clinical and pathologic staging was achieved. In this particular case, the minor staging change does not alter the patient’s treatment regimen. However, it is reasonable to assume that there might be instances where InVision can potentially assist prosectors in finding positive lymph nodes that could have been missed through use of manual palpation techniques alone; therefore, rendering consequential changes to staging and treatment options. Larger studies need to be completed to have a more thorough and accurate assessment of the effectiveness of InVision.
Conclusion:
Use of InVision improved lymph node retrieval by allowing the institution to meet the NCCN recommendation. It also impacted staging within the N category and decreased turnaround time through elimination of the need for re-grossing. While this is a single example of the value the innovative device provided, larger studies are being conducted to determine the impact on patient care and subsequent treatment decisions.
Authors
Rosalind Franklin University
Chicago, IL, United States
Wisconsin Diagnostic Laboratories
Milwaukee, WI, United States
Cision Vision Inc.
Mountain View, CA, United States
References
- Cision Vision Inc. https://cisionvision.com. Accessed May 2023.
- Amin MB, Edge SB, Greene FL, et al. AJCC Cancer Staging Manual 8th ed. Springer, 2018. Print.
- Li, Z., Huang, S., He, Y., et al. bioRxiv 2023.01.13.523938; doi: https://doi org/10.1101/2023.01.13.523938.
- National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology – Colon Cancer. Version 3.2022.
https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed March 2023. - Le Voyer TE, Sigurdson ER, Hanlon AL, et al. Colon cancer survival is associated with increasing number of lymph nodes analyzed: a secondary survey of intergroup trial INT-0089. J Clin Oncol 2003;21:29122919. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12885809.